
|
|
|
Scaphoid Fractures
What are scaphoid fractures?
The scaphoid bone is one of eight small bones that make up the" carpal bones" of the wrist. There are two rows of bones, one closer to the forearm (proximal row) and the other closer to the hand (distal row). The scaphoid bone is unique in that it spans the two rows (see Figure 1). This puts it at extra risk during injury, which accounts for it being the most commonly fractured carpal bone by far.
How do scaphoid fractures occur?
Fracture of the scaphoid bone occurs most frequently from a fall onto the outstretched hand. Typically there is pain initially, but the pain may decrease after days or weeks. Bruising is rare, and swelling may be minimal. Since there is no deformity, many people with this injury mistakenly assume that they have just sprained their wrist, leading to a delay in seeking evaluation. It is common for people who have fractured this bone to not become aware of it until months or years after the event.
Diagnosis of scaphoid fractures
Scaphoid fractures are most commonly diagnosed by x-rays of the wrist. However, when the fracture is not displaced, x-rays taken within the first week may not reveal the fracture. A non-displaced scaphoid fracture could thus be incorrectly diagnosed as a "sprain" because the x-ray was "negative". Therefore a patient who has significant tenderness directly over the scaphoid bone (which is located in the hollow at the thumb side of the wrist, or "snuffbox") should be suspected of having a scaphoid fracture and be splinted (see Figure 2). The patient should be re-evaluated about two weeks later, and if findings are still suspicious for a scaphoid fracture, x-rays at that time will usually show the fracture due to changes in the bone at the edge of the fracture. In cases where waiting two weeks in a splint may cause undue hardship, or if the x-rays remain negative but the clinical exam is still suspicious, more sophisticated (and expensive) imaging techniques may be utilized, such as CT scan, bone scan, or MRI.
Treatment of scaphoid fractures
If the fracture is non-displaced, it could be treated by immobilization in a cast. The cast usually covers the forearm, hand, and thumb, and sometimes includes the elbow for the first phase of immobilization. Although the fracture may heal in as little as 6 weeks, the healing can often be delayed. One reason for this delay is the variable blood supply to different parts of the scaphoid bone. The fracture can disrupt the bone's blood supply, impairing the healing. Part of the bone might even die after fracture due to loss of its blood supply, particularly in the proximal third of the bone, the part closest to the forearm. If the fracture is in this zone, or if it is at all displaced, surgery is more likely to be recommended. With surgery, a screw or pins are inserted to stabilize the fracture, often with a bone graft to help heal the bone (see Figure 3). Sometimes screw fixation surgery is recommended —even in non-displaced cases —so as to avoid prolonged casting.
Complications of scaphoid fractures
The term" chronic" refers to an old injury of greater than several months to years. If there is no or minimal cartilage damage, the ligament may be reconstructed as discussed above. If there is moderate to severe cartilage damage (arthritis), symptoms may be pain, stiffness, and swelling. These may be first treated with splinting and non-steroidal anti-inflammatory medicines, and later with cortisone injections. If these treatments fail, surgery may be an option. This may be a partial wrist fusion, removal of arthritic bones ("proximal row carpectomy"), wrist replacement, or complete wrist fusion. Your doctor will determine the best course of treatment.
Associated injuries
Non-union: If a scaphoid fracture goes unrecognized, it often will not heal. Sometimes, even with treatment, it may not heal because of poor blood supply. Over time, the abnormal motion and collapse of the bone fragments may lead to mal-alignment within the wrist and subsequent arthritis. If caught before arthritis has developed, surgery may be performed to try to get the scaphoid to heal.
Avascular necrosis: A portion of the scaphoid may die because of lack of blood supply, leading to collapse of the bone and later arthritis. Again, if arthritis has not developed, surgery to try to restore circulation to the bone may be attempted.
Post-traumatic arthritis: If arthritis has already developed, salvage-type procedures may be considered, such as removal of degenerated bone or partial or complete fusion of the wrist joint.
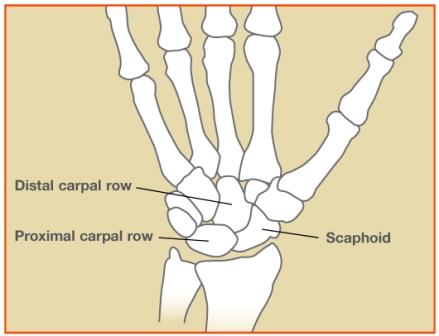
Figure 1: The scaphoid bone is unique in that it spans the two rows of wrist bones.
Figure 2: Significant tenderness directly over the scaphoid bone (which is located in the hollow at the thumb side of the wrist).
Figure 3: A screw or pins are placed to stabilize the fracture.
© 2006 American Society for Surgery of the Hand
|
|
|
|

|

Linden Oaks Medical Campus
10 Hagen Drive., Suite 310
Rochester, NY 14625
Ph: 585-922-5840
Rochester General Hospital
Parnell Office Building
1445 Portland Avenue,
Suite G-01
Ph: 585-922-5840
Park Ridge Hospital
1561 Long Pond Road,
Suite 216
Rochester, NY 14626
Ph: 585-368-4879
|
|





